
Malaria is a parasitic infection transmitted by the female Anopheles mosquito, infecting humans and insects alternatively. Caused by four Plasmodium species (P vivax, P falciparum, P ovale and P malariae), malaria is a public health problem in 90 countries around the world, affecting 300 million people and responsible directly for about one million deaths annually. Africa accounts for 90% of the mortality burden for malaria and South-east Asia accounts for 9% of the burden. Bangladesh is considered as one of the malaria endemic countries in South Asia. World Health Organization (WHO) considers malaria to be a major public health concern in Bangladesh. Malaria was nearly eradicated from the country by the 1970s but never disappeared in the eastern regions which are associated with tea gardens and forests. It re-emerged as one of the major public health concerns in the 1990s and remains so.
Malaria is one of the major public health problems in Bangladesh. The number of malaria cases in Bangladesh fluctuates seasonally. Malaria epidemics take place mostly in parts of the hilly and forested areas including the foothills. These areas are still with increased transmission potentials, due to prevailing vector prevalence, geophysical conditions and climate, and the presence of some ‘Hot-spots’ with perennial transmission round the year. The majority of these cases occur in the thirteen districts close to and/or bordering India and Myanmar. These thirteen districts, out of the 64 administrative districts of Bangladesh, are recognized as malaria endemic. Ninety-eight percent of the malaria case reports come from these thirteen districts. Three out of these thirteen districts, Bandarban, Khagrachari, and Rangamati, collectively known as the Chittagong Hill Tracts (CHT) districts, report the highest incidence of malaria within the country. These thirteen districts are difficult to reach due to the hilly terrain and therefore have inadequate passive surveillance and information systems resulting in poor reporting of malaria cases by the Ministry of Health, Government of Bangladesh [1-3].

Fig 1. Malaria Endemic areas in Bangladesh [3]
icddr,b was requested to conduct a cross-sectional survey in 2007-2008 with the largest NGO in Bangladesh, BRAC, and the Government of Bangladesh, to identify the prevalence of malaria. GFATM funded BRAC to implement a malaria control program in the 13 malaria-endemic districts to reduce the burden of malaria in Bangladesh, including both preventative and curative measures. ICDDR,B found that the overall malaria prevalence in these 13 districts was 3.1% and it was significantly higher in children. The prevalence of Falciparum malaria in children up to 4years was as high as 8.5% and between 5 and14 years, 6.6%. In Khagrachari district, however, the average prevalence was over 15%. Understanding this spatial distribution of malaria, identifying geographic risk factors and the population at risk are important steps toward effective malaria control and targeted interventions in high-risk areas can significantly control malaria. A lack of proper data to date has prevented targeted interventions from taking place in any of these endemic districts yet.
Figure 2 shows a dramatic decline in both malaria cases (65% blue line) since 2008, and malaria deaths (92% red line) since 2007. This is largely the result of a very effective malaria control program.
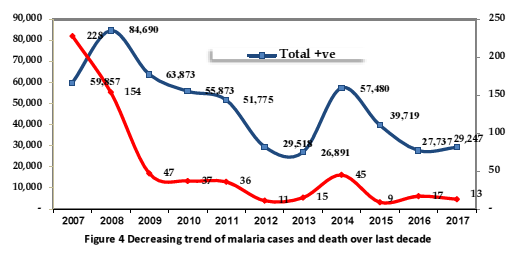
Fig 2: The decreasing trend of malaria cases and death over the last decade
But it means that it is very difficult to determine the attribution of climate change to levels of malaria. And that situation will remain. The malaria situation in Bangladesh is somewhat different from many other countries because the endemic areas tend to be at the country’s highest altitudes. This means that as temperatures rise due to global warming, and it might be expected that the suitable range (24-28 degrees C) for both the mosquito host (Anopheles) and the parasite (plasmodium) might be extended upwards, that will not be possible unless they relocate to more mountainous regions outside Bangladesh.
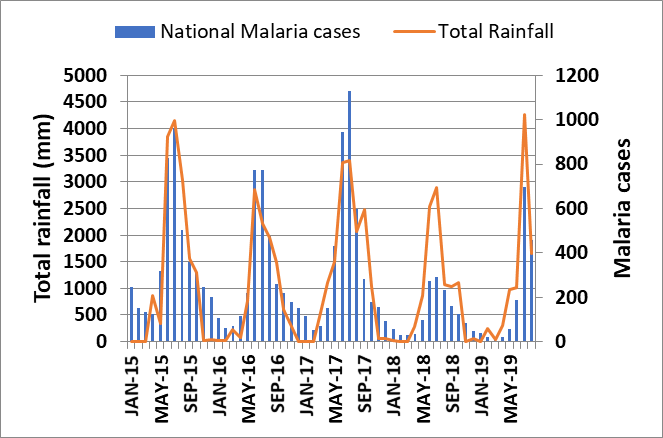
Fig 3: Rainfall vs. Malaria Cases
Figure 3 shows that malaria case numbers match rainfall patterns, it does not necessarily imply that if monsoon rainfall becomes heavier then numbers will increase. Humidity also plays a role.